Self knee Massage
Self Knee Massage Video I have been featuring essential oils in my regular newsletters and blogs. A couple of months ago I featured rosemary and a blend of rosemary, eucalyptus and black pepper and suggested…
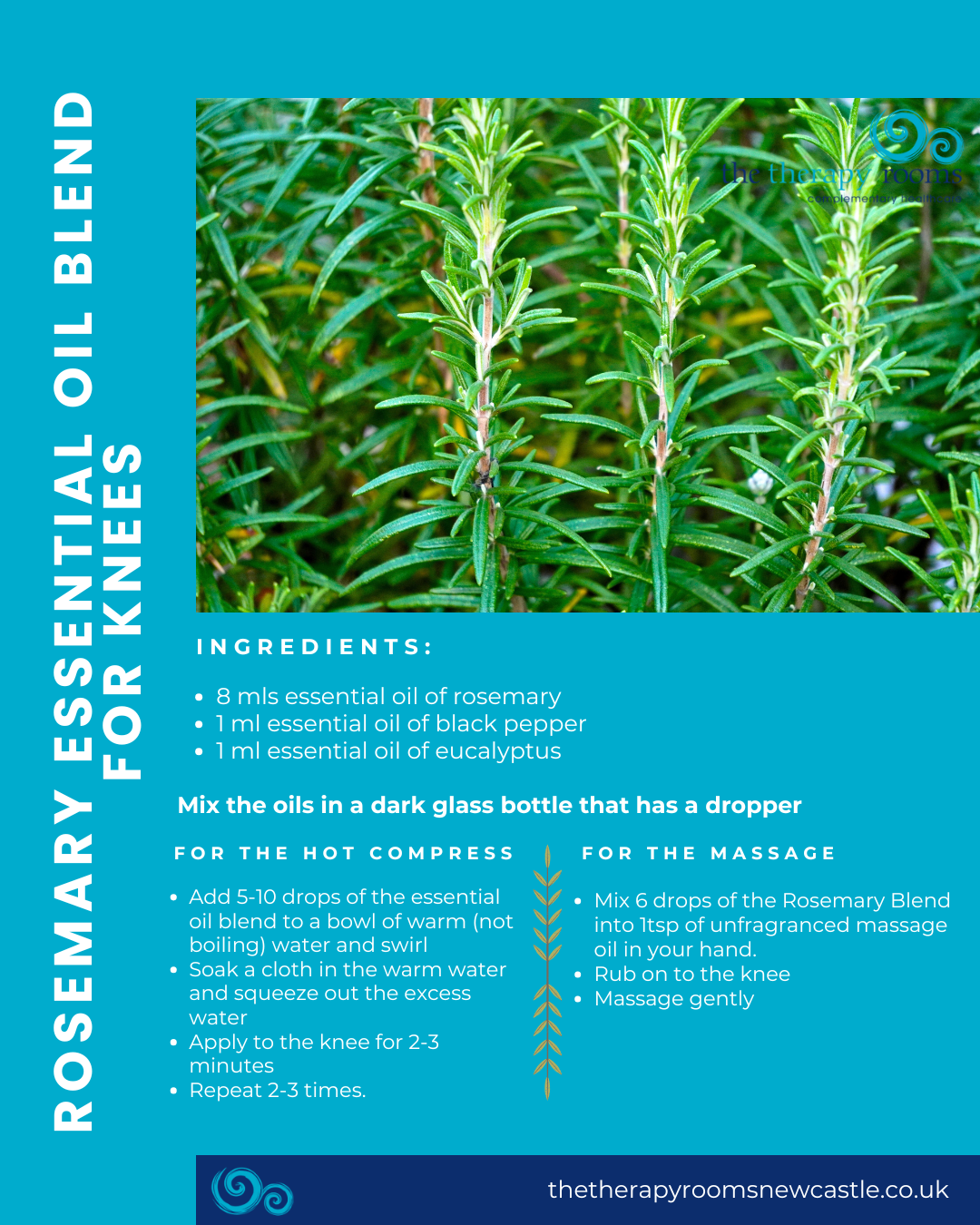
Self Knee Massage Video I have been featuring essential oils in my regular newsletters and blogs. A couple of months ago I featured rosemary and a blend of rosemary, eucalyptus and black pepper and suggested…

Is there a cure for Arthritis ? Arthritis can affect people of all ages and is a condition that is characterised by joint pain and inflammation. At present there is no cure for arthritis. Arthritis –…
Health Benefits Ginger Have you ever looked in to the health benefits ginger? It really has some fantastic benefits. Ginger can come in many forms Fresh Dried Powder Juice or as an Essential Oil. Health…

Slipped disc – can it be managed osteopathically? Spinal disc lesions are a very common occurrence, with an estimated 50-60% of the population having one or more bulging discs in their spine. However, only a…
Tracy at The Therapy Rooms Newcastle shows you how to get rid of shoulder pain How many times do you catch yourself hunching your shoulders at your desk? Look around. How many of your colleagues…
My journey started about five years ago. As a massage therapist, I was increasingly aware that the range of movement in my hips was poor. But as a reduction in range of movement is often gradual,…
Good computer posture is something that we’re all aware of, but only when we remember it. The computer: one of the most common tools in modern life… … and a device which forces the user…
In my article about knees, I mentioned that knee problems can be associated with the quadriceps muscles ‘switching off’. I wasn’t terribly happy with this state of affairs – as a big fan of how…
As massage therapists, we often see clients with painful knees. Professionals working with knees often bandy around the term VMO as the possible cause of the pain but what exactly does it mean. It stands…
No, nothing to do with guns and aiming, although Trigger Point Therapy – as anyone who has experienced it will testify – is far from painless! A Trigger Point is defined as ‘A hyper-irritable spot…